One year ago, I explored whether minimal residual disease (MRD) testing was entering its golden era in the war against cancer. In many ways, the momentum was unmistakable: Advances in circulating tumor DNA (ctDNA) detection, growing payer support and expanding use across hematologic malignancies and solid tumors signaled a shift from academic promise to clinical reality.
Today, the conversation has evolved. The question is no longer just whether MRD matters, but how we can extract maximum clinical value from these ultrasensitive signals. In 2026, artificial intelligence (AI) is emerging as the critical force multiplier that is turning raw detection capability into reliable, actionable intelligence for oncologists and drug developers alike.
The Persistent Challenges MRD Still Faces
Even with impressive technological progress, MRD testing in solid tumors continues to encounter real-world friction. Low tumor shedding, sequencing noise, biological variability and the inherent difficulty of distinguishing true cancer signals from background noise all limit broader adoption, particularly in early-stage disease in which timely intervention could make the biggest difference.
Tumor-informed approaches often deliver excellent specificity, but they require available tissue and time for customization. Tumor-naïve methods provide faster deployment, but have historically involved some trade-offs in sensitivity. On top of that, interpreting longitudinal data across heterogeneous patients remains challenging for busy oncology teams.
These are precisely the kinds of complex, data-intensive problems in which thoughtfully applied AI can make a meaningful difference. And not by replacing biological insight or clinical judgment, mind you, but by amplifying what the technology can achieve.
Taking MRD Technologies into the AI Age
What stands out in 2026 is the growing emphasis on multi-modal AI models that integrate multiple data streams rather than relying on ctDNA alone. These systems combine longitudinal ctDNA dynamics with clinical variables, digital pathology images, methylation patterns, fragmentomics and broader genomic context to build richer, more predictive risk profiles.
Companies at the forefront are making tangible progress here. Tempus has embedded its xM MRD and monitoring assays within a broader AI-driven clinico-genomic ecosystem and leverages vast real-world data to support more personalized treatment decisions and smarter clinical trial design. Meanwhile, Guardant Health continues to refine its Reveal assay through InfinityAI capabilities, while enhancing performance in tissue-free settings.
On the academic research front, platforms such as MRD-EDGE, developed by the Landau Lab at Weill Cornell Medicine, use machine-learning (ML)-guided signal enrichment and error suppression to extend detection limits even in low-shedding tumors. Early results across lung, breast, colorectal and melanoma cases suggest these methods can flag molecular recurrence months earlier than standard approaches.
AI is also helping address practical bottlenecks. In flow cytometry-based MRD analysis for blood cancers, AI-assisted workflows have significantly reduced manual review times and data analysis, while preserving or improving accuracy.
What stands out in 2026 is the growing emphasis on multi-modal AI models that integrate multiple data streams rather than relying on ctDNA alone.
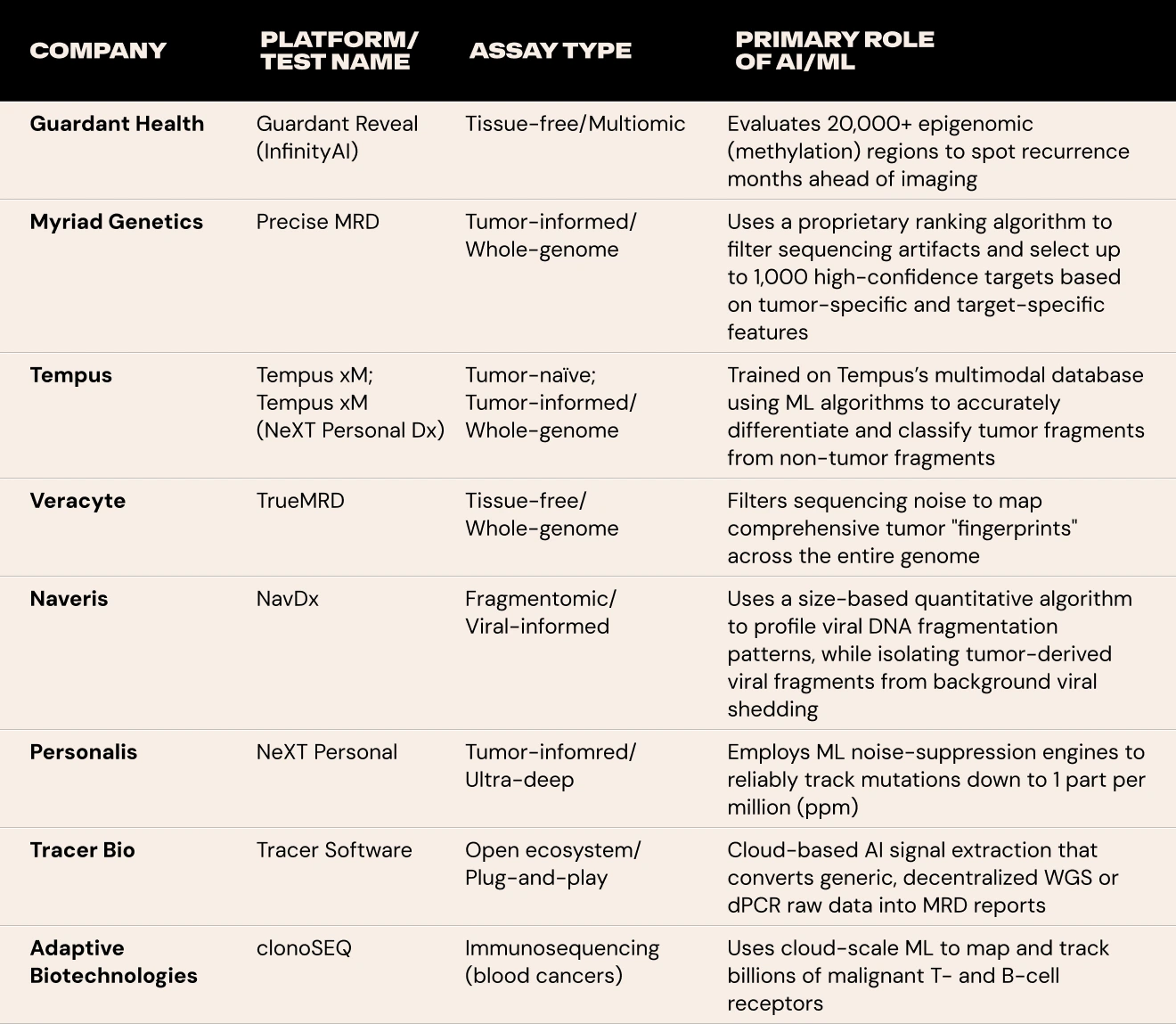
Here is a breakdown of a few leading MRD companies and platforms leveraging AI to monitor cancer recurrence today.
Real Progress in Solid Tumors
Compared with solid tumors, hematologic malignancies have had a head start in MRD adoption because malignant cells circulate in the blood, enabling direct and highly sensitive detection. In solid tumors, residual disease signals in plasma are more indirect, heterogenous and often scarce. AI-enhanced platforms are helping close the gap in MRD adoption for solid tumors by improving performance of blood-based MRD assays under far more challenging conditions.
Guardant Health’s work with Reveal stands out. Recent large-scale data in stage III colon cancer, published in the Journal of Clinical Oncology, demonstrated that the tissue-free test more precisely stratifies recurrence risk after surgery compared to traditional staging alone. Patients with detectable ctDNA faced substantially higher rates of recurrence and poorer survival, even among those with otherwise favorable pathologic features. This kind of evidence is helping shift MRD from a research tool toward routine postoperative decision-making.
Tempus is taking a different, but complementary, approach with its xM portfolio, offering tumor-informed and tumor-naïve options integrated into a data-rich platform. By combining MRD insights with multimodal real-world evidence, the company aims to support not just detection but ongoing therapy monitoring and adaptive strategies across solid tumors.
Myriad Genetics, for its part, is executing a focused commercialization strategy with Precise MRD. The company began a limited clinical launch in breast cancer in early 2026, with plans to expand into colorectal and renal cancers. This move targets community oncology settings, in which most cancer care occurs, and reflects a pragmatic push to make advanced MRD testing more accessible beyond major academic centers.
Collectively, these efforts are generating earlier lead times on recurrence detection, which, in turn, opens the door to more timely therapeutic interventions or, equally important, more confident treatment de-escalation in patients showing deep molecular responses.
Remaining Realities on the Ground
As someone who has followed many promising technologies through the Gartner hype cycle in this industry, I believe it’s essential to remain practical. AI in MRD is delivering real gains. However, it is not a panacea, and several important hurdles still need to be addressed before it reaches its full potential.
Data bias and generalizability remain concerns. Models trained predominantly on certain patient populations or data sources may not perform as well across diverse groups, which could exacerbate existing disparities in care. Interpretability is another key issue, in which oncologists need to understand and trust the reasoning behind AI-generated risk scores rather than treating outputs as black boxes.
Regulatory and clinical validation requirements are also evolving. Prospective studies that clearly link AI-improved MRD detection to meaningful improvements in survival or quality of life will be critical for broader reimbursement and adoption. On the practical side, integrating these advanced insights into existing clinical workflows without adding undue complexity or burden continues to be a challenge for many practices.
Finally, questions of equity and access cannot be overlooked. The most sophisticated AI-based MRD approaches risk remaining concentrated in well-resourced centers unless cost structures, infrastructure and implementation support improve.
Collectively, these efforts are generating earlier lead times on recurrence detection, which, in turn, opens the door to more timely therapeutic interventions or, equally important, more confident treatment de-escalation in patients showing deep molecular responses.
Looking Forward
Looking ahead, AI appears poised to help drive several important shifts in how MRD is used. We may see tighter integration between MRD monitoring and multi-cancer early detection frameworks, thereby creating more seamless care across the patient journey. Adaptive clinical trial designs that use AI-refined MRD as a dynamic biomarker could accelerate development timelines and improve patient selection for novel therapies.
There is also potential for more personalized “fingerprint” monitoring approaches that evolve with a patient’s disease over time, as well as hybrid decision-support tools that combine liquid biopsy data, imaging and clinical information into unified, actionable recommendations.
The ultimate goal remains using these capabilities to enable smarter, more precise (and ultimately kinder) cancer care that only intervenes when needed, thereby sparing patients unnecessary toxicity when the data support de-escalation.
Closing Thoughts
Last year’s post asked whether MRD was entering its golden era. In 2026, AI is helping write the next chapter that can benefit patients and inform smarter drug development by turning improved sensitivity into practical clinical utility. AI-based MRD technology is not replacing human judgment. In fact, it is giving oncologists, biopharma teams and diagnostics leaders even sharper tools for better decisions.
At HDMZ, we continue to help innovative companies, such as those advancing MRD, tell these complex, evolving stories with clarity and impact. Science is moving quickly, and the opportunity to meaningfully improve cancer outcomes has rarely been greater.